
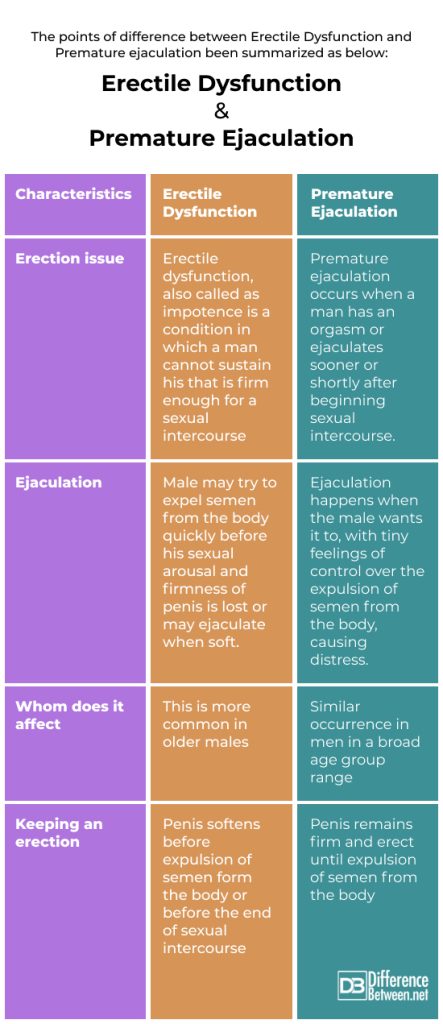
Premature ejaculation (PE) and erectile dysfunction (ED) are two of the most common male sexual disorders. While they are distinct conditions—PE involving early climax and ED involving difficulty achieving or maintaining an erection—they often share overlapping psychological and physiological factors. Understanding whether these conditions frequently occur together is important for accurate diagnosis and effective treatment.
Here we explores the relationship between PE and ED and the implications for men’s sexual health.
Prevelance of coexistence of PE and ED
The coexistence of PE and ED is relatively common and has been reported in multiple clinical studies. While prevalence rates may vary depending on definitions and populations studied, research indicates a significant overlap between the two conditions.
Prevalence of Coexistence:
- 20% to 30% of men with PE also report experiencing ED.
- Conversely, 30% to 50% of men with ED may also report symptoms of PE.
- One large international study (the MALES study) found that 29% of men with ED also experienced PE symptoms.
- A 2016 meta-analysis reported that the coexistence rate ranges from 17% to 36%, depending on age and diagnostic criteria.
Key Factors Influencing Coexistence:
- Age: Older men are more likely to experience both conditions.
- Psychological factors: Anxiety, performance pressure, and depression contribute to both PE and ED.
- Shared risk factors: Conditions like diabetes, cardiovascular disease, and hormonal imbalances are linked to both.
Clinical Relevance:
The high prevalence of coexistence highlights the need for comprehensive sexual health assessments. Treating one condition without addressing the other may lead to suboptimal outcomes or recurrence of symptoms.
Mechanism of Coexistence of Premature Ejaculation (PE) and Erectile Dysfunction (ED)
The coexistence of PE and ED is multifactorial and often results from complex interactions between psychological, neurobiological, and vascular mechanisms. While each condition can exist independently, they frequently influence and exacerbate each other.
1. Psychogenic Mechanism
- Performance Anxiety: Fear of losing erection can cause men to rush intercourse, leading to premature ejaculation.
- Low Sexual Confidence: Repeated episodes of either PE or ED can cause stress, which contributes to both conditions.
- Learned Behavior: Men with ED may develop PE over time as a subconscious attempt to achieve orgasm before losing their erection.
2. Neurobiological Mechanism
- Shared Neurotransmitter Pathways: Both conditions involve serotonin and dopamine dysregulation.
- Low serotonin: Associated with PE due to reduced ejaculatory control.
- Impaired nitric oxide signaling: Affects erectile function and may impact ejaculatory timing.
- Penile Hypersensitivity: In some cases, heightened penile sensitivity can contribute to PE and make maintaining an erection more difficult.
3. Vascular and Endocrine Mechanisms
- Vascular Insufficiency: Poor penile blood flow contributes to ED and may indirectly lead to PE by causing anxiety and a desire to climax quickly.
- Hormonal Imbalance: Low testosterone levels can affect libido, erection quality, and ejaculatory latency.
4. Medication and Substance Use
- Use of PDE5 inhibitors (e.g., sildenafil): Sometimes prescribed for ED, they may unmask or worsen PE if not managed properly.
- Substance abuse: Alcohol or stimulants can impair both erection quality and ejaculatory control.
5. Behavioral Feedback Loop
- ED causes anxiety → leads to PE
- PE results in frustration → worsens ED
This creates a vicious cycle, reinforcing the coexistence of both conditions.
Treatment of coexisting PE and ED
When PE and ED occur together, treatment should be comprehensive and individualized, addressing both conditions simultaneously to break the cycle that often links them.
**1. Initial Assessment
- Detailed medical and sexual history
- Psychological evaluation for anxiety, depression, or relationship issues
- Hormonal and metabolic screening if indicated (e.g., testosterone levels, diabetes)
**2. Pharmacological Treatment
a. PDE5 Inhibitors (for ED)
- Examples: Sildenafil (Viagra), Tadalafil (Cialis), Vardenafil
- Improve erection quality and reduce performance anxiety.
- May indirectly improve PE by increasing confidence and reducing the urge to climax quickly.
- Often used as first-line therapy when both ED and PE are present.
b. SSRIs (for PE)
- Selective serotonin reuptake inhibitors (e.g., Paroxetine, Sertraline, Fluoxetine)
- Delay ejaculation by increasing serotonin activity.
- Daily or on-demand use.
- Can be combined with PDE5 inhibitors when needed.
c. Topical Anesthetics (for PE)
- Lidocaine-prilocaine creams or sprays
- Reduce penile sensitivity and prolong ejaculation.
- Useful as adjunct therapy if hypersensitivity is a factor.
d. Combination Therapy
- PDE5 inhibitors + SSRIs is commonly used and well-tolerated.
- Target both ED and PE simultaneously.
- Some fixed-dose combinations (e.g., dapoxetine + sildenafil) are available in certain regions.
3. Psychosexual Therapy
- Cognitive Behavioral Therapy (CBT) for anxiety, depression, or relationship issues
- Sex therapy for performance anxiety and improving communication between partners
- Useful as adjunct to pharmacologic therapy, especially when psychological factors are significant
4. Behavioral Techniques (for PE)
- Start-stop technique
- Squeeze technique
- Kegel exercises to strengthen pelvic floor muscles
5. Lifestyle Modifications
- Regular exercise, weight loss, and smoking cessation
- Limiting alcohol and managing chronic conditions like hypertension or diabetes
- Improves overall sexual function
6. Hormonal Therapy (if indicated)
- Testosterone replacement therapy (TRT) for men with confirmed low testosterone
- Should be used cautiously and only after thorough evaluation
Treatment Strategy Summary:
| Condition | First-line Treatment | Secondary/Adjunct Treatment |
| ED + PE | PDE5 inhibitors | SSRIs, topical anesthetics, therapy |
| Psychogenic ED/PE | Psychotherapy/CBT + PDE5i/SSRI | Behavioral techniques |
| Hormonal causes | Hormonal therapy | Combined with other treatments |
Summary
Premature ejaculation and erectile dysfunction are the two most common male sexual disorders and often coexist in the same individual. Studies show that 20–50% of men with one condition may experience the other.
Key Points:
- High Prevalence: A significant number of men report symptoms of both PE and ED, particularly as they age or in the presence of psychological stress or chronic illness.
- Shared Mechanisms: Psychological factors (e.g., performance anxiety), neurotransmitter imbalances (e.g., serotonin, dopamine), and vascular or hormonal issues may contribute to both conditions.
- Vicious Cycle: ED may lead to anxiety and rushed intercourse, triggering PE. In turn, PE may cause performance pressure, worsening ED.
- Treatment Approach: A combined strategy is most effective:
- PDE5 inhibitors (e.g., sildenafil) for ED
- SSRIs or topical anesthetics for PE
- Psychotherapy and behavioral techniques for psychological contributors
- Lifestyle modifications and treatment of underlying health issues
- Importance of Holistic Management: Addressing both PE and ED simultaneously leads to better outcomes, improved sexual satisfaction, and reduced psychological distress.
Prof. Dr. Emin ÖZBEK
Urologist
Istanbul – TURKIYE

Leave a Reply